
Ergonomics
Common musculoskeletal injuries in dental practice
Lelia Lui and Bonnie Chung
Learning Objectives
Explain theoretical foundations underpinning common musculoskeletal injuries in dental practice.
List common musculoskeletal injuries in dental practitioners.
Principles
Dental practitioners often maintain static and uncomfortable positions to perform procedures requiring great precision. Prolonged static posture, repetitive movements and poor positioning can result in musculoskeletal disorders (MSD). MSDs are injuries or disorders of the muscles, nerves, tendons, joints, cartilage, and spinal discs. These cumulative microtrauma and repetitive use of awkward positions may result in muscular imbalance, neuromuscular inhibition, pain and dysfunction. Other factors influencing MSD's include genetic disposition, stress, physical health and environmental factors such as dental chairs, equipment, lighting and availability of a dental assistant.
Natural curvature of the spine
It is important to appreciate that the spine is made up of four natural curvatures: cervical lordosis, thoracic kyphosis, lumbar lordosis and sacral kyphosis. Movement in the sacral kyphosis is limited due to the fused vertebrae, however, the lumbar and cervical spine are quite mobile and can be easily affected. Changes in any part of the curvature of the spine affect the other areas. If one curvature becomes more exaggerated or flattened, the alignment of the vertebrae can no longer be assisted by gravity to rest on top of each other in a balanced manner. The spine begins to depend on its associated muscles, ligaments and soft tissue to maintain erect.
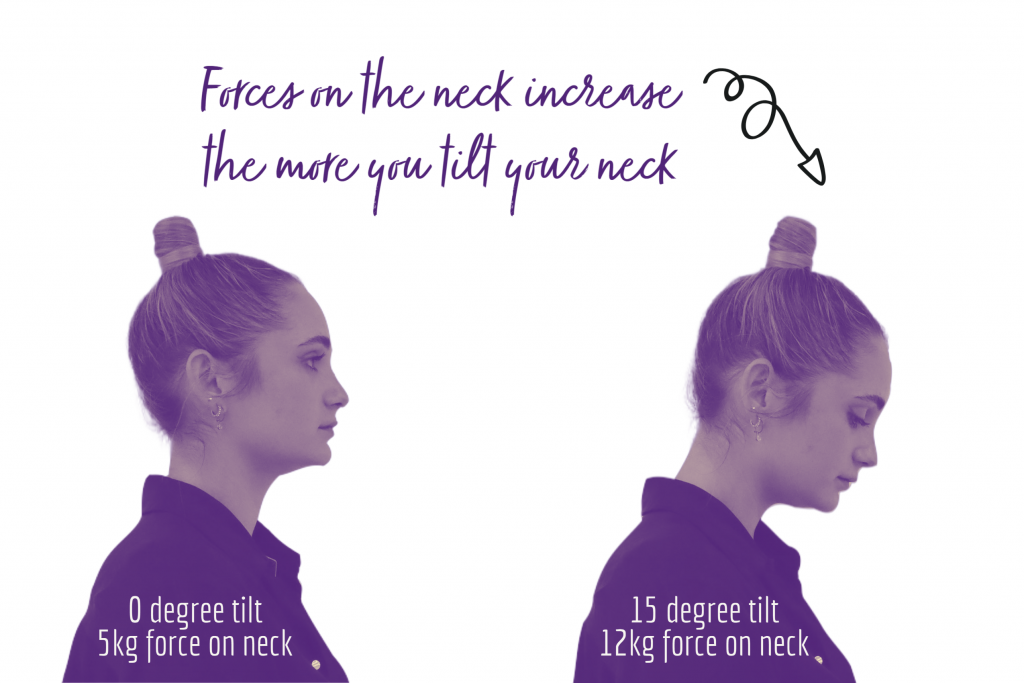
In the cervical spine, for every 2.5 cm the head moves forward, it gains 0.45 kg in weight for the muscles in the upper back and neck to support its position. Similarly, another study calculated the weight of a full-grown head in different angles of cervical flexion. The head weighs almost 5 kg in the neutral position. Forces on the neck more than the double to approximately 12kg when the head is tilted to 15◦. Vasavada et al. also found that mechanical demand on extensor muscles increases 3-5 times during seated tablet computer use versus seated neutral posture.[1]
Prolonged static postures
A static posture is when more than half of the body’s muscles contract to hold the body in a motionless position against gravity. Static positions require more effort from muscles compared to dynamic movements. Prolonged static posture leads to muscle fatigue and imbalance between the stabilising and dynamic muscles.
In a prolonged static posture, synovial fluid production is reduced which results in joint hypomobility. The function of synovial fluid is to provide joint lubrication. A loss of mobility can lead to degenerative changes. A flexed seated posture increases loading on the facet joint of the lumbar vertebrae which leads to degenerative changes such as it contributes to lower back pain. The spinal disks provide movement and transmits forces in between vertebrae. Unsupported sitting increases the pressure in lumbar disks by 40% compared to standing, but in a flexed forward and rotated posture, the pressure increases by 400%. The spinal disc is made up of several areas with the nucleus pulposus in the centre encircled by the annulus fibrosis. The posterior portion of the annulus fibrosis is the thinnest. A repeated forward flexed posture would lead to the nucleus pulposus to push against the posterior annulus fibrosis. This can lead to weakening and tearing of the annulus fibrosis and eventual disc bulge or herniation. As only the outer third of annulus fibrosis is innervated, by the time pain is felt, it means that the damage would have exceeded two thirds of the structure.
Forward posture
Repeatedly forward leaning leads to overuse of lower back extensors but weakens the deep stabilising abdominal muscles such as the transversus abdominis which has a protective role in low back pain prevention. The increased use of lower back extensor muscles such as the lumbar erector spinae leads to ischaemia due to the decreased muscle oxygenation as the muscle needs to contract harder to maintain the posture. The tendon stretches and compresses the vascular supply leading to depletion of nutrients and oxygen. The increased contraction also leads to lactic acid and other metabolite accumulation leading to inflammation and pain. Without allowing these muscles to rest in a prolonged static posture, the body utilises muscle substitution as a protective mechanism which can lead to joint hypomobility, nerve compression and disorders of the spinal disc. Ischemic areas are likely to develop trigger points which are groups of muscle fibres that are in a constant contracted state that feels like a knot within a muscle. When these trigger points are pressed, it may cause local or referred pain.

Practical application to the dental environment
Common MSDs in dental team members involve the neck, shoulders, arms and wrists. Previous studies have suggested that more than half of the workforce experience some type of pain due to MSD and it leads to loss of work and productivity for dental practitioners. Common injuries include low back pain, tension neck syndrome, trapezius myalgia and rotator cuff impingement and carpal tunnel syndrome. In Australia, the prevalence of MSD for the dental professions was 82%, and over two thirds reported experiencing pain.[2] The majority of dentists (87.2%) reported experiencing at least one MSD in the last year and one in ten reported taking sick leave for an MSD. MSD is a significant occupational health issue for the dental profession.[3]
Hand and wrist injuries develop when musculoskeletal structures cannot withstand the cumulative work activity stresses. An example of this includes constant flexion and extension or awkward movements of the wrist and the fingers. In severe cases, muscle atrophy and pain can prevent an individual from working. A significant wrist and hand MSD includes Carpal Tunnel Syndrome, which is the compression of the median nerve within the carpal tunnel of the wrist causing volar wrist pain with numbness and tingling in the distribution of the median nerve (thumb, index finger, middle finger and radial side of the ring finger). The pain can radiate to the forearm, elbow and shoulder. Repeated movement at the wrist or sustained pinch-gripping an instrument with inadequate rest.
A common awkward posture dental practitioners assume is the forward bending and repeated upper body rotation to one side. Right handed operators often rotate their neck to the left and side bend to the right for better visibility. The muscles on the side of the body rotate and becomes stronger and shorter, whereas the opposing muscles become ischemic and painful. The imbalance in forces is also exerted onto the spine leading to reduced range of movement in one direction.[4]
Operators may place themselves into a forward head posture with rounded shoulders, as the patient is in front of them below eye-level. This prolonged static posture may elongate and weaken the stabilising shoulder muscles which include middle and lower trapezius, rhomboid and serratus anterior muscles. This further reinforces pulling of the shoulder blades away from the spine which achieves a rounded shoulder posture long term. Similarly, the head is pulled forward because the anterior “mover” muscles, such as the scalenes and sternocleidomastoid, become shortened and overactive, while deep neck flexor muscles are weakened. A cycle of muscle imbalance is created when the ligaments and muscles adapt to this new position which makes it uncomfortable to return to the correct position.
Nerve entrapment disorders
| Disorder | Description | Mechanism |
| Carpal Tunnel Syndrome | Compression of the median nerve within the carpal tunnel of the wrist. | Repeatedly bending hand up, down or from side to side at the wrist and continuous pinch gripping an instrument without resting the muscles. |
| Ulnar Neuropathy | Compression of ulnar nerve when it passes through the wrist. | Bending hand up, down and from side to side at the wrist and holding the little finger a full span away from the hand. |
| Pronator Syndrome | Compression of median nerve at the elbow between pronator teres. | Holding the arms away from the body. |
| Thoracic Outlet Syndrome | Compression of the brachial nerve plexus and vessels between the neck and shoulder. | Forward head tilting, forward shoulder hunching and continuous overhead reaching. |
Disorders of the neck and back
| Disorder |
Description |
Mechanism |
|
Tension Neck Syndrome |
Pain, stiffness or tightness in the neck, shoulders or upper spine. |
Prolonged static posture, forward flexed posture, repeated extreme arm reaching, elevated arms and tensed shoulders. |
|
Cervical Spondylosis |
Age-related wear and tear of the cervical spinal disc relating to formation of bony overgrowths. |
Prolonged, repeated forward flexed posture. |
|
Cervical Disc Herniation |
Tearing of the annulus fibrosis of the disc leading to the herniation of the nucleus pulposis which could impinge on the spinal cord |
Prolonged, repeated forward flexed posture. |
|
Lumbar Radiculopathy |
Compromise of the lumbar spine nerve root, with majority of the cases caused by herniated disc. |
Poor ergonomics, prolonged static posture or sitting. |
|
Non-specific/ Mechanical Low Back Pain |
It can develop without a clear mechanism of injury and often a pathoanatomical diagnosis could not be made. Pain, distress and disability can be associated with repeated strain or even in the absence of any tissue strain. |
Poor ergonomics, prolonged static posture or sitting. |
Disorders of the shoulders
|
Disorder |
Description |
Mechanism |
|
Trapezius Myalgia |
Pain, stiffness or tightness in the upper trapezius muscle. |
Static and prolonged elevation of shoulders, forward head posture. |
|
Rotator Cuff Tendonitis |
Inflammation of tendons in the shoulder region. |
Holding the elbow above waist level and holding the upper arm away from the body. |
Tendonitis
|
Disorder |
Description |
Mchanism |
|
De Quervain’s syndrome |
Stenosing condition of the first dorsal compartment which comprises the extensor pollicis brevis and the abductor pollicis longus tendons at the base of the thumb and wrist. |
Constant tight gripping, repetitive thumb abduction. |
|
Tendonitis |
Inflammation of the tendons of the wrist resulting from strain. |
Repeatedly extending the hand up or down at the wrist. |
|
Tenosynovitis |
Inflammation of the tendons on the side of the wrist and at the base of the thumb. |
Hand twisting, forceful gripping, bending the hand back or to the side. |
|
Epicondylitis |
Inflammation of the tendons that bend your wrist backward away from your palm. |
Holding elbows constantly in acute angle away from torso. |
|
Extensor Wad Strain |
Injury of the extensor muscles of the thumb and fingers. |
Extending the fingers independently of each other. |
Key Takeaways
- Prolonged static posture, repetitive movements and poor positioning are the crux for injury risk and the cumulative damage caused leads to muscular imbalance, pain and dysfunction.
- In dentistry, the most damaging habits are forward bending with upper body rotation to one side as well as repeated wrist movements with constant pinch gripping of instruments.
- MSDs can lead to reduced productivity and can lead to loss of work for dental practitioner
- Valachi B, Valachi K. Preventing musculoskeletal disorders in clinical dentistry: strategies to address the mechanisms leading to musculoskeletal disorders. The Journal of the American Dental Association. 2003 Dec 1;134(12):1604-12. ↵
- Marshall ED, Duncombe LM, Robinson RQ, Kilbreath SL. Musculo-skeletal symptoms in New South Wales dentists. Aust Dent J 1997;42: 240–246. ↵
- Leggat PA, Smith DR. Musculoskeletal disorders self-reported by dentists in Queensland, Australia. Aust Dent J. 2006 Dec;51(4):324-7. doi: 10.1111/j.1834-7819.2006.tb00451.x. PMID: 17256307. ↵
- Bhandari SB, Bhandari R, Uppal RS, Grover D. Musculoskeletal disorders in clinical dentistry and their prevention. Journal of Orofacial Research. 2013:106-14. ↵
Injuries or disorders of the muscles, nerves, tendons, joints, cartilage, and spinal discs.
When more than half of the body’s muscles contract to hold the body in a motionless position against gravity.
